
In shoulder arthroscopy, portals are not just incisions—they are the foundation of every successful procedure. These small, carefully crafted entry points dictate a surgeon’s ability to visualize, navigate, and treat complex shoulder pathologies. From repairing torn labrums to addressing rotator cuff tears, the art of portal creation is what separates haphazard exploration from targeted, efficient surgery. This article delves into the critical role of portals, their anatomy, variations, and the technical nuances that make them indispensable in modern arthroscopy.
Why Portals Matter: The Key to Access and Control
Portals serve as the surgeon’s “eyes and hands” inside the joint. Poorly placed portals lead to:
- Limited visualization (e.g., struggling to see the anterior labrum).
- Instrument collision (“sword fighting” between tools).
- Iatrogenic damage (e.g., scuffing cartilage or snagging tendons).
Optimal portal placement ensures a clear view, ergonomic instrument movement, and minimal soft tissue disruption.
Anatomy of Portals: Navigating the Shoulder’s Safezones
-
-
-
- Every portal must balance access with safety, avoiding nerves, vessels, and tendons.
-
-
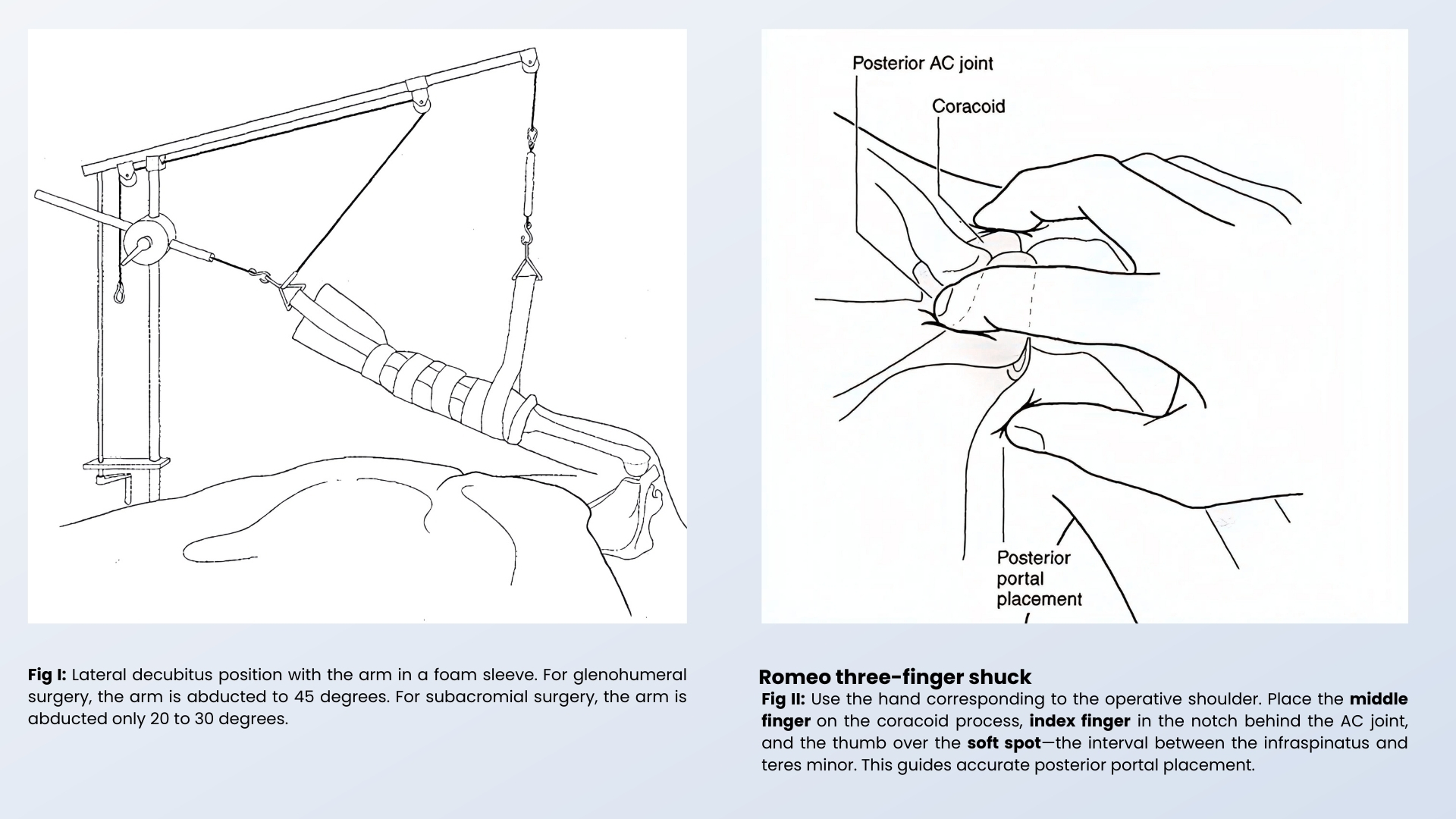
Table 1: Standard Portals
| Portal Name | Location | Purpose | Key Risks |
| Posterior | 2 cm inferior/medial to posterolateral acromion | Primary viewing portal for glenohumeral joint | Axillary nerve (if too low) |
| Anterior | Lateral to coracoid process | Labral repair, debridement | Musculocutaneous nerve, cephalic vein |
| Lateral | 2–3 cm lateral to acromion | Subacromial decompression, rotator cuff | None if placed correctly |
Table 2: Accessory Portals
| Portal Name | Location | Purpose | Key Risks |
| 5 o’clock | Anteroinferior transubscapular | 1) Bankart repair (inferior glenoid anchors) | Axillary nerve |
| 7 o’clock | Posteroinferior | 1) Posterior labral repair
2) Loose body removal 3) 7 ‘0’ clock anchor insertion |
Axillary nerve |
| Neviaser | Superior, posterior to AC joint | 1) Suture passage SLAP repair
2) Rotator cuff repair – Supraspinatus |
Suprascapular nerve/artery |
| Portal of Wilmington | Posterolateral, 1 cm lateral to posterolateral acromion | 1) Anchor insertion
2) SLAP/rotator cuff repair using trans-tendinous approach |
Suprascapular nerve (if too medial) |
| Posterolateral | Lateral to posterior portal | 1) Rotator cuff footprint visualization
2) Best portal for Rotator Cuff Repair |
Axillary nerve (if too inferior) |
| High Postero- Medial | 2-3 cm inferior to the spine of the scapula and 2-3 cm medial to the posterior portal | 1) Infraspinatus Repair with Penetrating Hook | Axillary nerve and artery |
| Subclavian portal | Anteriorly and superior, 1 to 2 cm medial to the coracoid and inferior to the clavicle. |
1) Anterior Supraspinatus Repair with Penetrating Hook | Very close to Neurovascular structure |
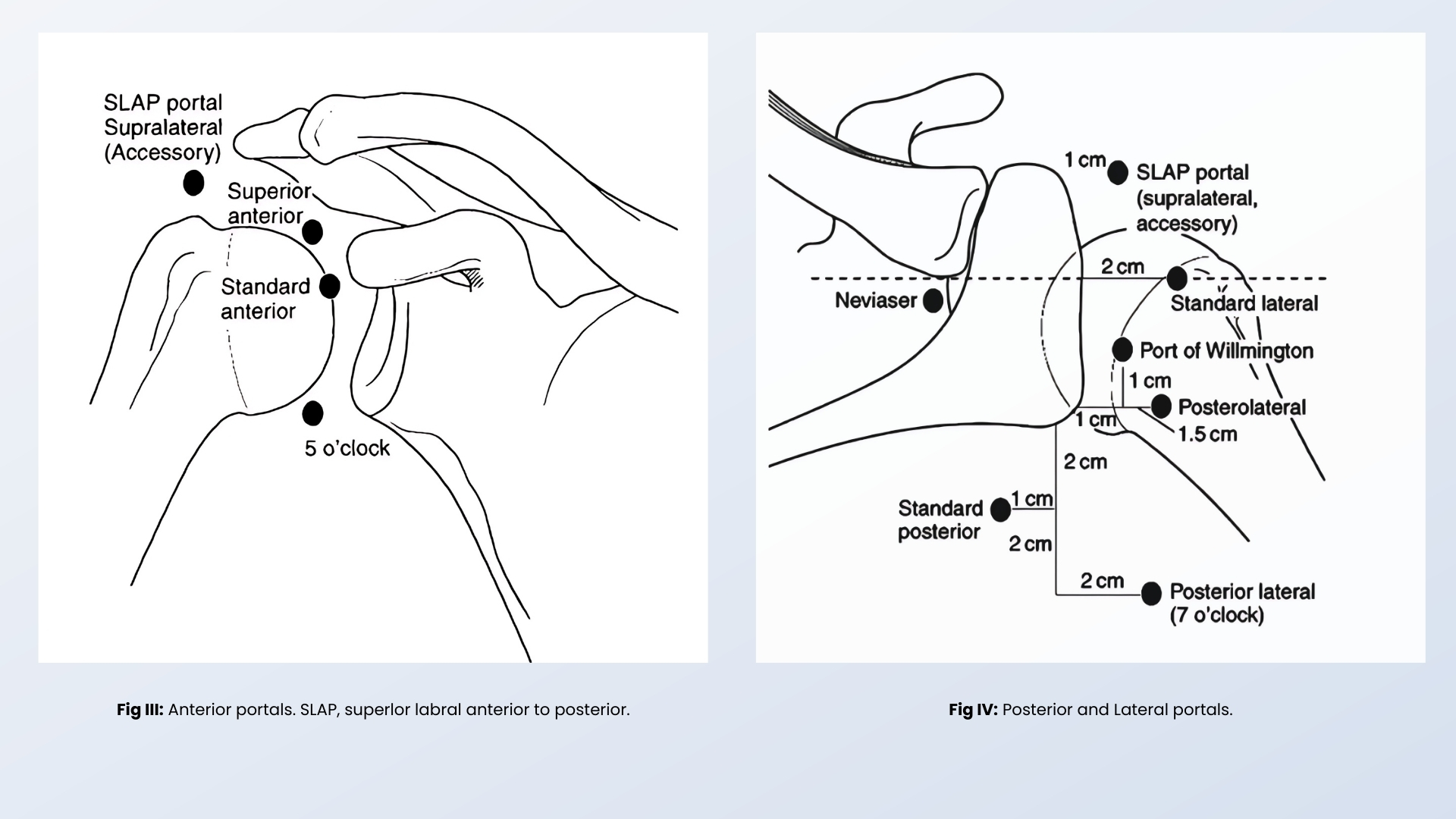
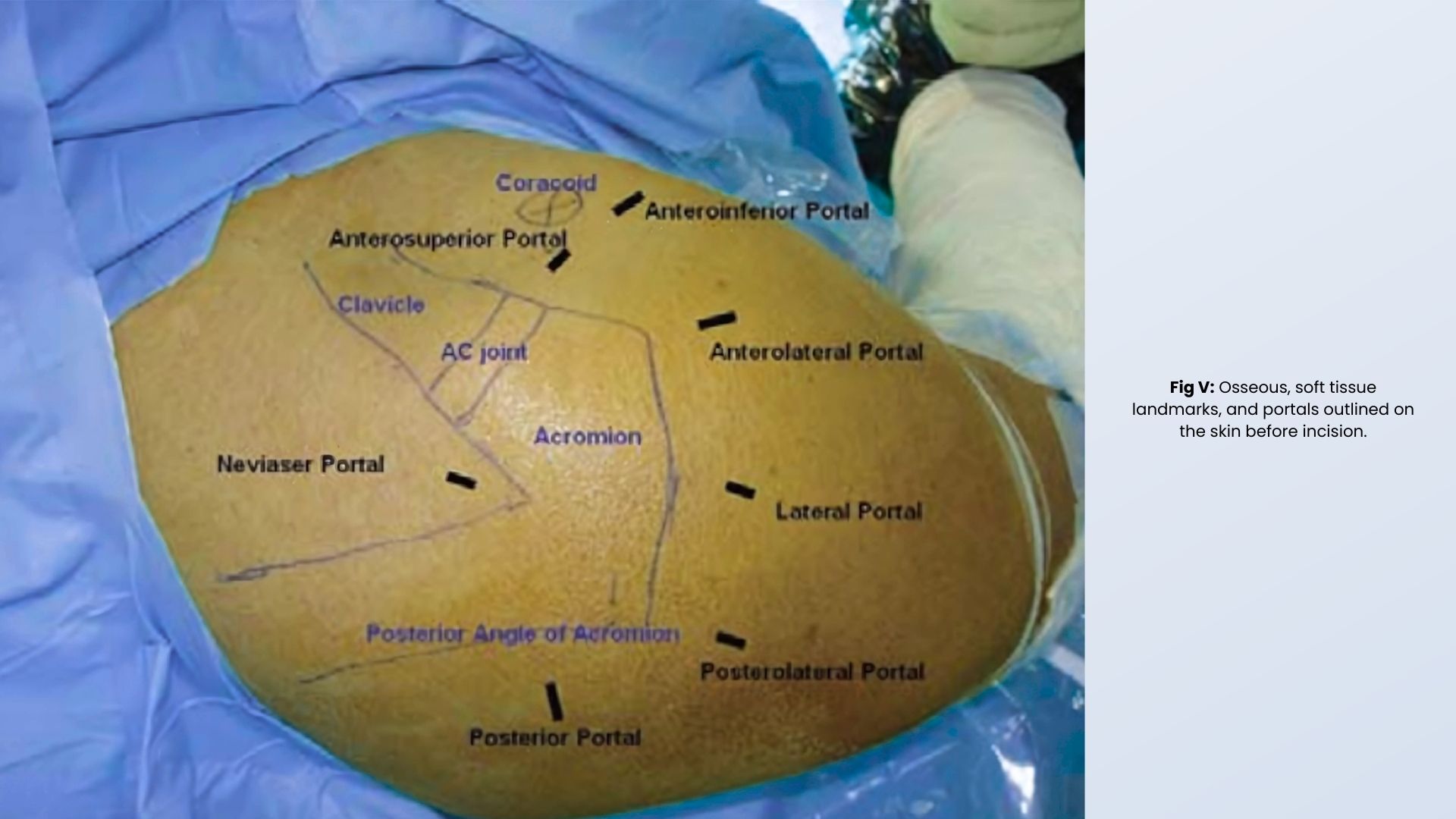
Table 3: Portal Techniques
| Technique | Description |
| Spinal Needle Localization | Test trajectory with a needle before incision to avoid errors. |
| Blunt Trocar Insertion | Use a blunt trocar to enter the joint, minimizing soft tissue damage. |
| Inside-Out Method | Push a switching rod from inside the joint to create a new portal. |
| Outside-In Method | Insert a needle into the joint first, followed by a cannula over a wire. |
Table 4: High-Risk Zones: Avoiding Pitfalls
| Structure at Risk | Location |
Prevention Tip |
| Axillary Nerve | 5 o’clock, 7 o’clock, posterolateral | Avoid portals below the equator of the glenoid. |
| Suprascapular Nerve/Artery | Neviaser, Portal of Wilmington | Keep portals lateral and superior. |
| Cephalic Vein | Anterior portals | Stay lateral to deltopectoral groove. |
Key Tips for Safe Portal Creation
- Always palpate bony landmarks (acromion, coracoid) before incising.
- Use fluid pressure (20–30 mmHg) to expand the joint and reduce cartilage damage.
- Blunt dissection > sharp dissection to minimize bleeding and nerve injury.
- When in doubt, use a needle first to confirm angles and depth.
Why Portals Are Everything
Portals define what you can (and can’t) fix in shoulder arthroscopy. A well-placed portal means:
- ✅ Clear vision of the pathology.
- ✅ Smooth instrument movement without collisions.
- ✅ Lower risk of complications.
Poor portals lead to frustration, prolonged surgery, and potential harm. Simplify your approach with these tables—they’re your cheat sheet to mastering the “GATEWAYS” of shoulder arthroscopy! 🔑