Anterior Cruciate Ligament (ACL) injuries are among the most common and devastating sports-related knee injuries. While ACL Reconstruction (ACLR) has become the gold standard of treatment, one key challenge persists — residual rotational instability.
Many patients, particularly young athletes in pivoting sports, continue to experience instability or re-injury despite technically successful ACLR. This is where Extra-Articular Tenodesis (EAT) comes in. By reinforcing the anterolateral aspect of the knee, EAT procedures provide additional control against tibial internal rotation, complementing ACLR and protecting the graft from overload.
Why is Extra-Articular Tenodesis needed?
Extra-Articular Tenodesis is a surgical technique performed outside the joint capsule to control excessive tibial rotation. Unlike intra-articular ACLR (which directly reconstructs the ACL), EAT focuses on the anterolateral complex (ALC) — a group of stabilizers that includes the iliotibial band (ITB), capsule, and the anterolateral ligament (ALL).
The principle is simple: add an extra reinforcement on the lateral side of the knee to:
- Eliminates the Pivot Shift: Directly counteracts abnormal rotational motion.
- Protects the ACL Graft: Offloads stress from the new ACL graft during healing, potentially reducing re-tear rates.
- Restores Confidence: Allows athletes to return to cutting and pivoting sports with greater trust in their knee.
Indications for EAT:
EAT is not necessary for all ACL reconstructions. It is particularly useful in:
- Revision ACL reconstruction (to protect the graft).
- High-grade pivot shift (Grade II–III).
- Young athletes (<25 years) in pivoting/cutting sports (football, basketball, rugby).
- Generalized ligamentous laxity (Beighton score ≥4).
- Chronic ACL deficiency with secondary instability.
- Cases with meniscal deficiency or root tears.
Surgical Options in EAT:
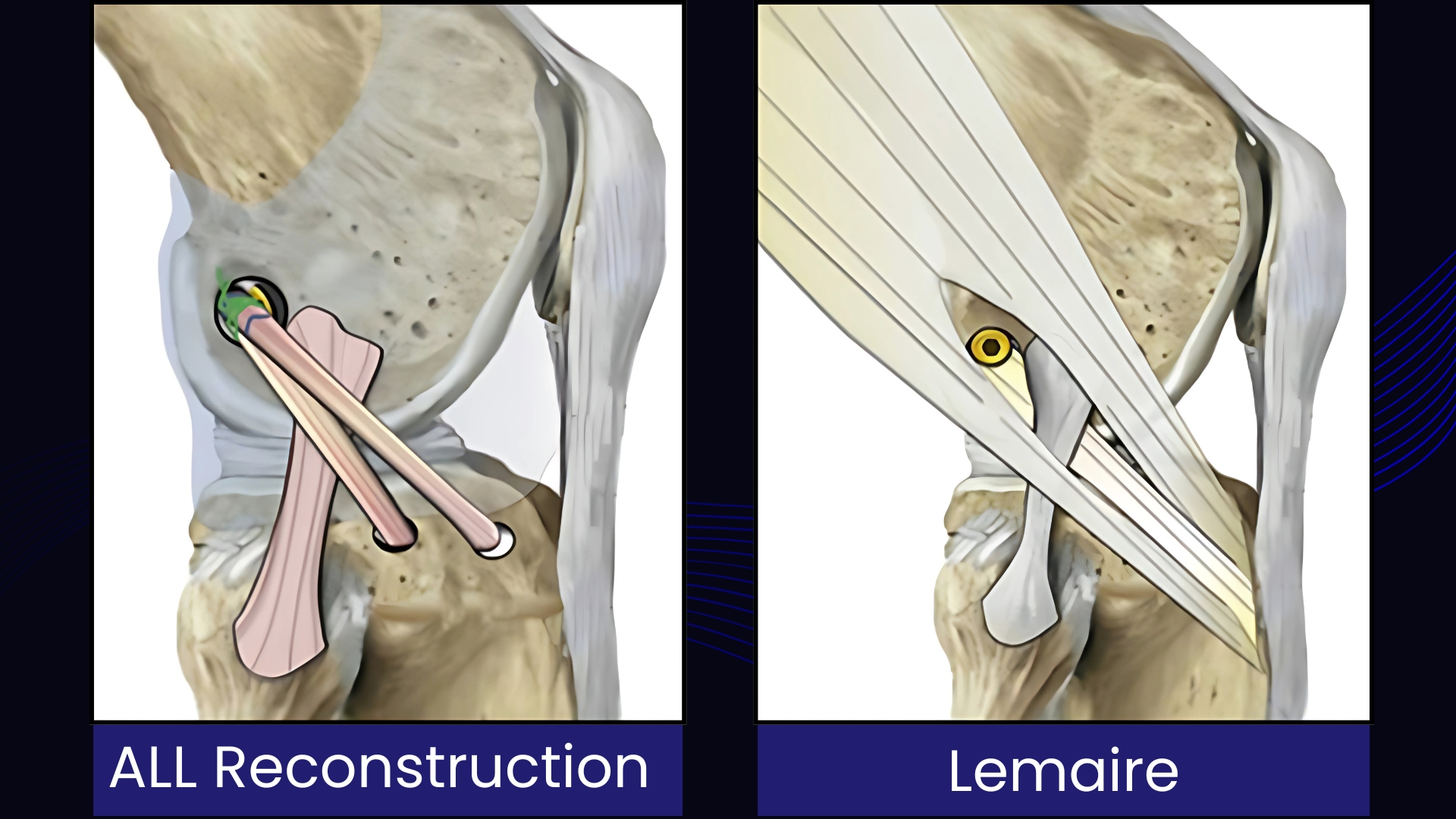
- Modified Lemaire ITB Tenodesis
- Anterolateral Ligament (ALL) Reconstruction
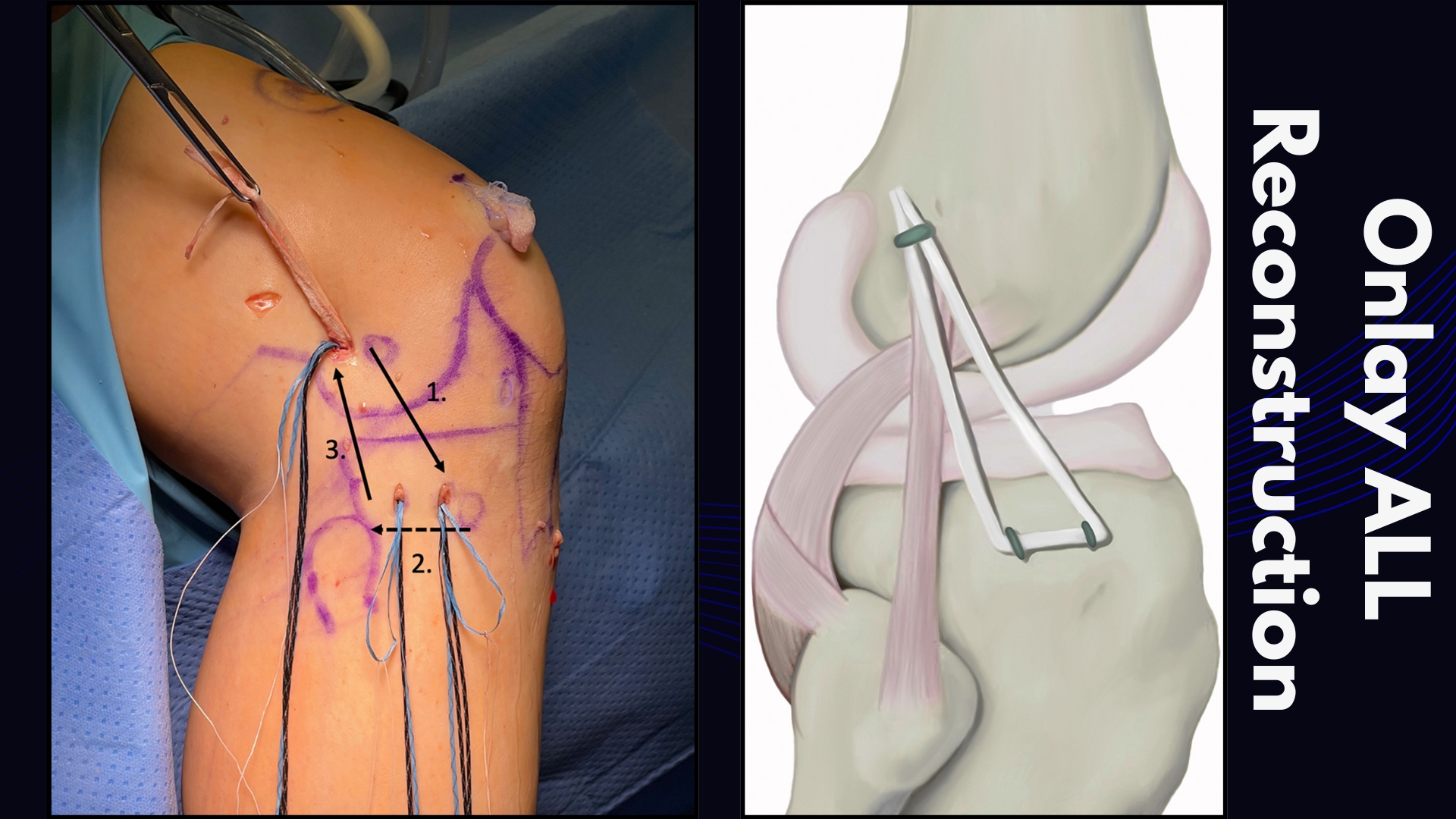
- Onlay ALL Reconstruction
Comparative Overview
| Technique | Modified Lemaire ITB Tenodesis | ALL Reconstruction | Onlay ALL Reconstruction |
| Graft Source | Iliotibial Band (ITB) | Gracilis/ITB | Gracilis/ITB |
| Fixation | Fixation to bone surface (tenodesis) | Full bone tunnel | Shallow socket (onlay) |
| Anatomical Accuracy | Non-anatomic (functional restraint) | Anatomical | Anatomical (simplified) |
| Fixation Method | Distal attachment to bone, proximal end fixed with staple/screw/anchor. | Proximal and distal ends fixed within bone tunnels. | Proximal end fixed to the surface of the bone with anchors/screws; distal end may be in a tunnel. |
| Primary Advantage | Proven, effective, and technically simpler. Avoids the need for a separate free graft. | Aims for a more precise anatomical reconstruction. | Avoids tunnel convergence with the ACL graft, a major technical benefit. |
| Tunnel Convergence Risk | Minimal | Higher | Minimal |
| Key Limitation | Risk of over-constraint | Risk of tunnel convergence | Graft specificity, technical complexity |
| Ideal Use Case | Primary & revision cases, high-grade pivot shift | Surgeons prioritizing anatomy, primary cases | Revision surgery, multi-ligament injuries, narrow femurs |
In Extra-Articular Tenodesis (EAT), fixation reliability is crucial, and Osteocare offers trusted solutions. The HealFix™ Knotless Anchor (4.75 & 5.5mm) enables secure knotless fixation with adjustable tensioning. The OsteoFix™-FD Titanium Anchor (5.0mm) provides dual-thread strength for firm cortical and cancellous purchase. For minimal bone removal, the OsteoKnot™ All Suture Anchor (3.0mm) ensures strong yet less invasive fixation. Complementing ACLR, the EcoButton™ delivers reliable femoral fixation. These solutions together empower surgeons to achieve stable, reproducible outcomes in EAT.

🔚 Conclusion
The story of Extra-Articular Tenodesis (EAT) reflects how surgical practice evolves with science and evidence. Once dismissed as outdated, EAT has re-emerged as a valuable complement to ACL reconstruction, addressing one of the most persistent problems in knee surgery — residual rotational instability.
Each technique brings its strengths:
- Modified Lemaire ITB Tenodesis remains a time-tested, effective option, particularly in young athletes and revision settings.
- ALL Reconstruction represents a precise, anatomical solution, restoring native biomechanics while minimizing over-constraint.
- Onlay ALL Reconstruction simplifies the procedure, offering practical advantages by avoiding tibial tunnel drilling while maintaining comparable stability.
The growing body of clinical evidence and biomechanical studies makes it clear that the future of ACL surgery is not “ACLR alone,” but ACLR combined with selective extra-articular augmentation.
Ultimately, the success of EAT lies in personalized decision-making: matching the right procedure to the right patient, balancing stability with mobility, and respecting individual demands such as sporting activity, age, laxity, and revision needs.
EAT is no longer a historical footnote — it is a vital part of modern ACL surgery, giving patients not just a stable knee, but the confidence to return to the activities they love.